Today, my clinical group learned how to start an IV!
Types of IV's:
1) Peripheral: the ones that go in your hand, arm, elbow... these can stay in for only 3 days.
2) PICC (Peripherally Inserted Central Catheter): these go on your arm as well, but the catheter travels all the way up to the heart. Like what Aunt Pam, Dad, and Matt had for Lyme.
3) Central Line: the one that goes in the jugular (IJ) or on the chest (subclavicular). These go straight to the heart too. Lines that go to the heart can stay in for up to a month or so.
4) Port a caths: these are surgically implanted under the skin in the chest and are accessed by a 90 degree (looks like an up-side down L)needle when the patient needs medicine or treatment. These can stay in for a year or longer.
There are so many rules to dealing with different IV lines; what you can give through them, what you can't. How you can administer the medicine, how you can't. How often you need to change the bandage, etc.
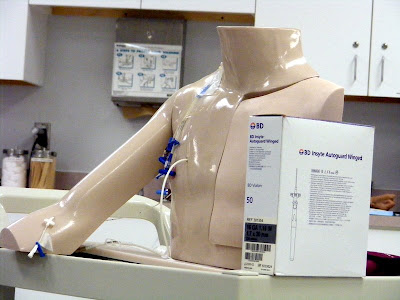
This guy has all the types of IV's, and we use him to practice IV dressing changes on. And see that box? Those are the needles we used to practice with!
An Angiocath is the basic IV line. It has the flixible catheter with a needle inside, after inserting the needle, you pull it out, leaving the catheter in the vein. The newer models of needles have a small white button that pulls the needle into itself when pushed after you have placed the IV. It's a safety feature: with this, there won't be an open needle on your field when you pull the needle out of the catheter. Here's how it works, watch for the uptake of the needle, it's fast!
Before we stuck eachother, we practiced our critical thinking skills with patient scenarios. We were each a "patient", and we went around the room figuring out what size needle was best to use (gauge 14,16,18,20, or 22?) for each condition, and where to put it (hand, forearm, or antecubital/elbow?).
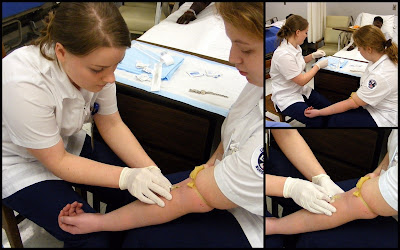
This is Melissa! She's one girl in my clinical group. She's playing a 15 year old athlete, who, based on her age and physicality, should have good veins. Because of this, you can think of using a larger size needle (the lower the gauge number, the bigger the needle/larger diameter needle). But, the patient is going to the OR, so you need to put at least a size 18. We chose a size 18 gauge on the right hand, this way the anesthesiologist can be on the one side while the OR surgeons, etc. are on the left side dealing with the leg.
Here was my scenario:
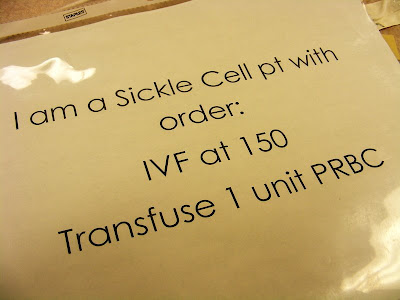
EEK! Sickle Cell is painful! So first, you need to ask
where the patient is having pain, because that is where the sickle cell crisis is, and what if they are having their crisis in their arm?? You would definitely want to avoid putting a
needle where someone is having a
crisis! Plus, she is getting PRBC (Packed Red Blood Cells) which means you would need a big lumen so the Red Blood Cells can pass through without being broken up.
Other scenarios also included a diabetic with dizziness and fainting (Her veins would be less-than-ideal because of the diabetes, but... what's the worse case scenario? Dizziness in a diabetic is from low blood sugar, and if it gets low enough she would need to be given Dextrose, which is really thick. So she needs a big lumen, 'round a 16 or 18). Also, a 50 year old with chest pain and nausea (heart attack! This requires TWO IV lines because he could code.) It was fun!
Next, we watched our teacher place an IV line so we could see how it's done.
Here's the whole process, in three parts (you can pause the music above so you can hear what the teacher is saying):
Don't you just wanna grab a 22 gauge, find a forearm, and go nuts?!
Well if you do, here's what you'll need:

A tourniquet, alcohol preps, a needle (pink is size 20, a smaller needle), tegaderm (a clear "plastic bandage" that will cover the IV site, keep it stable, but still let you assess it every 2 hours without having to take the bandage off), some tape, some gauze, and a saline flush (the outside tube with a blue end, where the saline flushes or medicine is pushed into). Don't forget the gloves! All the needles are color-coded depending on their size. We usually see blue (22), pink (20), and green (18).
Here's a vein we can practice on first. You can see if you go straight through the vein with this device, and it helps you visualize what is happening under the skin.

In this picture, the pliable catheter is in the vein, and the needle is coming out.
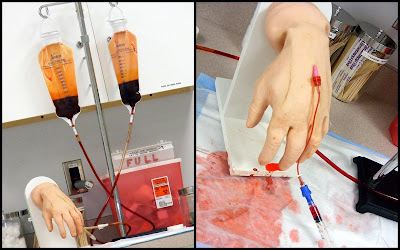
Now we can move onto the practice arms. These are pretty realistic. They actually BLEED!! And there are many veins to choose from, so whichever one you stick, be sure to go low, go slow, and go like you know ;)
Here's Maya.

Here's a hand you can practice on too. Looks like Thing from the Adam's Family. This is my site that I put in. Look at all the blood (but that's not all from me, just the fresh-looking drip on the white board). See the blue tip? That's the "saline flush". You can hook up IV tubing and syringes there. Without it, the blood would just backflow out of the IV line and the patient would bleed all over the place. This would be terrible if the blue tip came off of a central line because it would be like the heart was spilling out on the floor.
Here I am having a go at the practice arm.
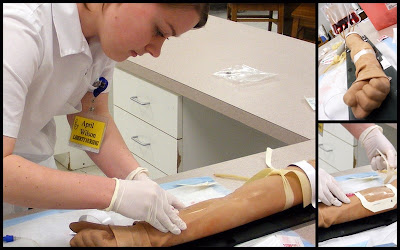
And finally, a real victim! I got it on the first try, no problems! It was an awesome feeling, I wasn't nervous or shaky while I was doing it.... but the second I was done inserting the line, my hands started to shake! I was so excited I had just done that!
Here's the whole clinical group! We've been together since day one of Junior year.
Don't worry about our arms, this was our "funny picture", so it's all fake blood.
We're nuts.
(Congratulations on getting to the end of the post! It was a doozie.)
 It's 10 minutes closer to campus than I am now! This is the living room, unfortunately the fire place doesn't work.
It's 10 minutes closer to campus than I am now! This is the living room, unfortunately the fire place doesn't work. Here's the kitchen:
Here's the kitchen: 
 This is the hallway off the living room that leads down to three bedrooms and a bathroom. My bedroom is the door straight ahead, just slightly to the left.
This is the hallway off the living room that leads down to three bedrooms and a bathroom. My bedroom is the door straight ahead, just slightly to the left.  It's pretty tiny, and I'm going to try to pull the carpet up and see if I can't store it downstairs, then put it back before we move out. It's really gross. But hey, it's my own room, right?
It's pretty tiny, and I'm going to try to pull the carpet up and see if I can't store it downstairs, then put it back before we move out. It's really gross. But hey, it's my own room, right?
 We will have access to the tennis court, "beach" area, and lake!
We will have access to the tennis court, "beach" area, and lake!











 You get to choose from 5 doors. The first on on the right will take you outside, which means you are going to get the mail, which means you are about to walk a really long way. No thanks. The double doors straight ahead will take you into the craft room, formerly known as the music room, until all the instrumets were taken out. This room will also connect you to the kitchen, but we'll get into that later.
You get to choose from 5 doors. The first on on the right will take you outside, which means you are going to get the mail, which means you are about to walk a really long way. No thanks. The double doors straight ahead will take you into the craft room, formerly known as the music room, until all the instrumets were taken out. This room will also connect you to the kitchen, but we'll get into that later. As you keep turning to the left, there is a doorway that takes you to the living room. (See the other door through the craft room? Go through it and immediately on your left is another doorway to the living room. Immediately to your right is a bathroom. Straight ahead is the kitchen.)
As you keep turning to the left, there is a doorway that takes you to the living room. (See the other door through the craft room? Go through it and immediately on your left is another doorway to the living room. Immediately to your right is a bathroom. Straight ahead is the kitchen.)

 Now here's walking into the living room. The door there on the right is the kitchen.
Now here's walking into the living room. The door there on the right is the kitchen.

 Now I'm standing in the kitchen, looking towards the guest room and the downstairs door.
Now I'm standing in the kitchen, looking towards the guest room and the downstairs door.
 Do you feel dizzy? Hope I didn't confuse you.
Do you feel dizzy? Hope I didn't confuse you. 









 On my dresser, I keep my printer and my class books. Those are ALL nursing books, plus 2 that you can't see in the picture :) I use them when I write my weekly profiles for clinical.
On my dresser, I keep my printer and my class books. Those are ALL nursing books, plus 2 that you can't see in the picture :) I use them when I write my weekly profiles for clinical.

 These are over-the-door hooks that I put on the walls using "Command Strips" as curtain holders. I still need one more for the other side.
These are over-the-door hooks that I put on the walls using "Command Strips" as curtain holders. I still need one more for the other side.  The view from the window this morning: SNOW! 8 inches last night.
The view from the window this morning: SNOW! 8 inches last night.

 I get to see these girls every morning!
I get to see these girls every morning! And these girls too! Elizabeth, Mandy, and Laura
And these girls too! Elizabeth, Mandy, and Laura

 My reminder for clinical: If you are missing your med cards or profile, you go home. Scarry!
My reminder for clinical: If you are missing your med cards or profile, you go home. Scarry!